Metabolism
on-line - the virtual tutorial room
copyright © 2008 - 2015 David A Bender
 Hyperammonaemic coma due to liver failure
Hyperammonaemic coma due to liver failure
Mr ABV has been jaundiced for several days, and has come to see his GP
What is the cause of the yellow pigmentation of the skin (and especially the whites of the eyes) in jaundice?
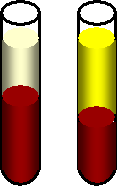 Jaundice
is due to accumulation of bilirubin the blood plasma, giving it and his skin
a yellow colour.
Jaundice
is due to accumulation of bilirubin the blood plasma, giving it and his skin
a yellow colour.
Jaundice can develop for two reasons:
when bilirubin arising from the catabolism of haem in old red blood cells is not conjugated in the liver
when the bile duct is obstructed (e.g. with gall stones) so that bilirubin cannot be excreted in the bile
The GP suspects that Mr ABV's problem is viral hepatitis, but also thinks that it may be due to alcoholic liver damage, because she can smell alcohol on his breath, and on abdominal examination his liver is palpable and firm. She takes blood samples for both standard liver function tests (measurement of liver enzymes in the blood plasma) and also immunology to test for viral hepatitis.
On questioning, Mr ABV says he only drinks a glass or two of whisky each evening, and the occasional glass of wine.
The immunology results come back negative. The liver function test results are shown in the table below.
| enzyme | Mr ABV | reference range |
| aspartate transaminase | 2500 units /L | < 40 units /L |
| alanine transaminase | 1000 units /L | < 50 units /L |
| gamma-glutamyl transpeptidase | 1200 units /L | < 60 units /L |
| alkaline phosphatase | 2500 units /L | < 120 units /L |
Why are the activities of these enzymes in plasma elevated in liver disease?
They have been released from dead and dying liver cells. They indicate the extent of liver damage, but have no function in the bloodstream.
Why is it important to know the Km of an enzyme in order to measure its activity in plasma?
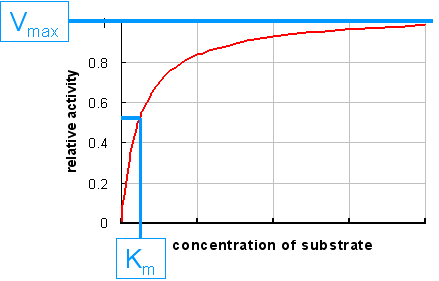 The amount
of an enzyme in plasma is measured by measuring its catalytic activity.
The amount
of an enzyme in plasma is measured by measuring its catalytic activity.
This means that the limiting factor in the assay must be the amount of enzyme that is present, and not the amount of substrate that is available for the enzyme to act on.
In other words, the enzyme should be more or less saturated with substrate, so that it is acting at its maximum rate (Vmax).
Saturation of the enzyme is achieved when the concentration of substrate is about 10 - 20x greater than the Km.
At lower concentrations of substrate the rate of product formation will depend on both the amount of enzyme present and the amount of substrate available, and the results will be meaningless.
In non-alcoholic liver disease the ratio of aspartate transaminase : alanine transaminase activities in plasma is < 1. In alcoholic liver disease it is > 2.
Do you think it is likely that Mr ABV is telling the truth when he says that he "only drinks a glass or two of whisky each evening, and the occasional glass of wine"?
No. The ratio of aspartate transaminase : alanine transaminase activities in his plasma is 2.5, which is strongly indicative of alcoholic liver disease, suggesting that he must be drinking considerably more than a glass or two of whisky each evening, and the occasional glass of wine
Why do you think the ratio of aspartate transaminase : alanine transaminase activities in plasma is so different in alcoholic and non-alcoholic liver disease?
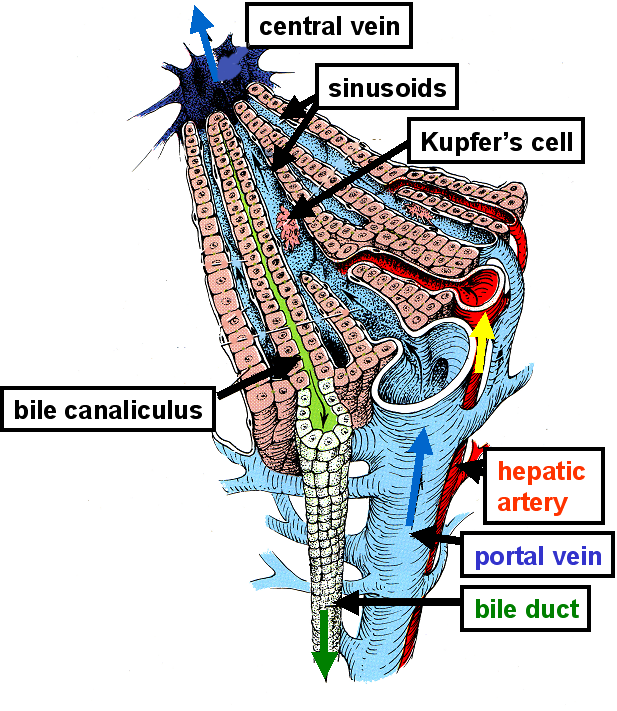 This
is the result of zonation in the liver.
This
is the result of zonation in the liver.
Hepatocytes in the region around the hepatic portal vein (periportal hepatocytes) have a different complement of enzymes from those around the central vein (perivenous hepatocytes), and notably have a higher content of aspartate transaminase than of alanine transaminase.
Alcohol reaches the liver through the hepatic portal vein, which drains the gut, and therefore will affect periportal hepatocytes more than those further away from the hepatic portal vein.
In non-alcoholic liver disease, cells throughout the liver, and not just those adjacent to the hepatic portal vein, are affected. Perivenous hepatocytes make up a considerably greater proportion of total hepatocytes than do periportal cells.
Bilirubin metabolism is summarised below:
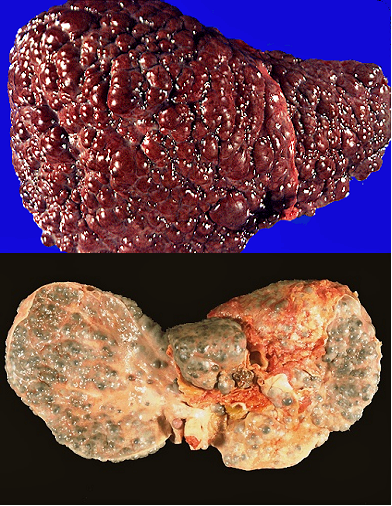
We now suspect that Mr ABV is a heavy drinker, and his jaundice is due to alcoholic liver disease. He has an enlarged liver with signs of cirrhosis.
The picture above on the left shows the surface anatomy of a cirrhotic liver, and below a cross section.
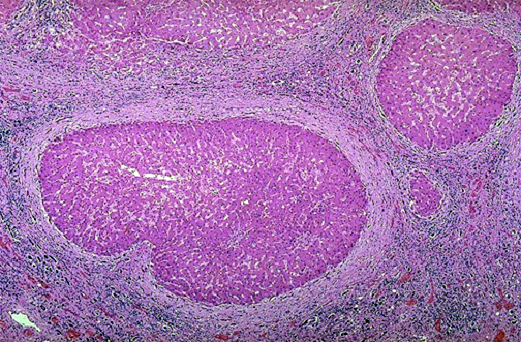
The picture on the right shows the histology of a cirrhotic liver, with regenerating hepatocytes surrounded by fibrous connective tissue.
Would you expect to find conjugated or unconjugated bilirubin in Mr ABV's plasma?
It will be unconjugated bilirubin - his is obviously in liver failure and his liver cannot conjugate the bilirubin that is formed by macrophages.
You would see conjugated bilirubin when jaundice is due to obstruction of the bile duct (e.g. by gall stones, pictured below)) because although the liver can conjugate bilirubin, it cannot be adequately excreted in the bile.


There is equilibrium between ammonia and ammonium ions in plasma:
![]()